Draft Annual report 2022
On this page
Skip the menu of subheadings on this page.This is a paper for discussion.
This does not represent the views of the Committee and should not be cited.

Image shows 5 blue hexagon shapes with blue text written across them. The text reads: Committee on Toxicity, Committee on Carcinogenicity, Committee on Mutagenicity.
Committee on Toxicity of Chemicals in Food, Consumer, Products and the Environment Annual Report 2022
About the Committees
This is the 32nd joint annual report of the Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment (COT), the Committee on Mutagenicity of Chemicals in Food, Consumer Products and the Environment (COM) and the Committee on Carcinogenicity of Chemicals in Food, Consumer Products and the Environment (COC).
The aim of these reports is to provide a brief background to the Committees' decisions. Those seeking further information on a particular subject can obtain details from the Committee’s statements and minutes, available from the websites listed below or from the Committee’s administrative Secretary.
In common with other independent advisory committees, Committee members are required to follow a Code of Conduct which also gives guidance on how commercial interests should be declared. Members are required to declare any commercial interests on appointment and, again during meetings if a topic arises in which they have an interest. If a member declares a specific interest in a topic under discussion, and it is considered to be a conflict of interest, he or she may, at the Chairman's discretion be allowed to take part in the discussion but is excluded from decision- making. Annex 1 contains the terms of reference under which the Committees were set up. The Code of Conduct is at Annex 2 and Annex 3 describes the Committees’ policy on openness.
Annex 4 is the Good Practice Agreement for Scientific Advisory Committees. Annex 5 contains a glossary of technical terms used in the text. Annex 6 is an alphabetical index to subjects and substances considered in previous reports. Previous publications of the Committees are listed at Annex 7.
These three Committees also provide expert advice to other advisory committees, such as the Scientific Advisory Committee on Nutrition, and there are links with the FSA Science Council, Veterinary Products Committee and the Expert Committee on Pesticides (formerly the Advisory Committee on Pesticides).
The Committees’ procedures for openness include the publication of agendas, finalised minutes, agreed conclusions and statements. These are published on the internet at the following links:
This report contains summaries of the discussions and links to the Committees’ published statements. Paper copies are available upon request to the Secretariats.
Preface

Head and soldier image of Prof Alan Boobis. Prof Boobis is photographed outside, they wear glasses and a pale striped shirt.
Text needed
Professor
Alan Boobis (Chair)
OBE PhD CBiol FRSB FBTS FBPhS
COT evaluations
Statement on the effects of Vitamin D on maternal health
1.1 In 2019, The Scientific Advisory Committee on Nutrition (SACN) agreed to conduct a risk assessment on nutrition and maternal health focusing on maternal outcomes during pregnancy, childbirth and up to 24 months after delivery; this would include the effects of chemical contaminants and excess nutrients in the diet. The Committee on the Toxicity of Chemicals in Food, Consumer Products and the Environment (COT) was consulted, and decided that Vitamin D should be considered for a detailed risk assessment.
1.2 There are two forms of vitamin D; these are vitamin D2 (also known as ergocalciferol) and D3 (also known as cholecalciferol). Vitamin D2 can be found in plants and fungi and therefore is only available to humans via the diet. Vitamin D3 is made in human skin via ultraviolet radiation from the sun, and can also be found in oil rich foods or supplements of animal origin such as cod liver oil. Vitamin D3 is reported to be about three times more potent than vitamin D2.
1.3 Both forms of vitamin D are converted in the body by the liver to analogous substances called 25-hydroxyvitamin D (25(OH)D) and the 25OHD is further converted in the kidney to analogous substances called 1,25-dihydroxyvitamin D (1,25(OH)2D); this is the active form of vitamin D.
1.4 Vitamin D (in reality two forms as described in paras 3-4) plays an important role in maintaining healthy bones by ensuring adequate uptake of calcium. It also helps maintain healthy muscles by aiding muscle contraction and helps nerves and the immune system to function. However, consuming too much vitamin D from food sources and supplements can cause adverse health effects.
1.5 Too much vitamin D in the body can lead to hypercalcaemia (higher than normal calcium levels in the blood), which can lead to hypercalciuria (higher than normal levels of calcium in urine), demineralisation of bones, kidney and cardiovascular issues. Other side effects of excess vitamin D may include vomiting, nausea, constipation and diarrhoea.
1.6 It is important to note that whilst too much vitamin D can be consumed from foods and supplements it is not possible to make too much vitamin D via ultraviolet radiation from the sun. This is because there are inbuilt biochemical mechanisms in our skin that prevent vitamin D3 reaching toxic levels from exposure via skin.
Effects of vitamin D during pregnancy and lactation
1.7 There is currently no information available on the adverse health effects that excess vitamin D might cause during the period preceding conception.
1.8 Information on the adverse health effects caused by excess vitamin D during pregnancy and lactation is limited, but hypercalcemia (higher than normal calcium levels in the blood) can occur during pregnancy, especially in individuals that have mutations in genes involved in vitamin D metabolism. Individuals with these mutations have experienced hypercalcemia after consuming up to 1,250 µg per month of vitamin D. Hypercalcemia during pregnancy may increase risk of fetal and neonatal morbidity. Excess vitamin D during pregnancy may also result in fetal and neonatal hypercalcemia, which can lead to adverse effects on the digestive system, behaviour and growth.
1.9 There is limited evidence for adverse health effects that could arise due to excess vitamin D exposure during lactation. However, hypercalciuria could possibly occur, with one clinical study reporting it in women that consumed supplements of 700 µg per week vitamin D. However, participants in this study had low levels of calcium before consuming the supplements that increased their levels to be in “possible hypercalciuria” range.
1.10 In 2003, the Expert Group on Vitamin and Minerals (EVM) set an intake level of 25 µg per day as the level of vitamin D that would not be expected to result in adverse health effects – i.e. a safe level of intake. More recently The European Food Safety Authority (EFSA) developed a tolerable upper limit (TUL) of 100 µg per day
for the general adult population, including pregnant women. This TUL was endorsed by the COT.
1.11 This risk assessment showed that women attempting conception, pregnant and lactating women who consume vitamin D only from food (and not supplements) are very unlikely to be at risk of adverse health effects from vitamin D as their exposure levels are below the TUL of 100 micrograms per day.
1.12 Only a minority of women attempting conception, pregnant and lactating women who consume vitamin D from both food and supplements are above the TUL of 100 micrograms per day. It is important to note that this would only be of health concern if their intakes were sustained long-term. Pregnant women with mutations in the genes involved in vitamin D metabolism may be more likely to experience adverse health effects such as high blood calcium levels and high calcium levels in the urine.
1.13 Ultimately the COT concluded that consumption of higher strength vitamin D supplements alone or in combination with food can result in exceedance of the TUL and pose a potential health concern. However, consumption of lower strength supplements that are aimed at pregnant and breast-feeding women, either alone or in combination with food is very unlikely to result in excess vitamin D intake or adverse health effects related to excess vitamin D intake.
1.14 The full COT statement can be found here: Statement 01/22 Vitamin D
Statement on the potential effects that excess iodine intake may have during preconception, pregnancy and lactation
1.15 The Scientific Advisory Committee on Nutrition (SACN) is currently conducting a risk assessment on nutrition and maternal health focusing on maternal outcomes during pregnancy, childbirth and up to 24 months after delivery; this would include the effects of chemical contaminants and excess nutrients in the diet.
1.16 The Committee on Toxicity was consulted, and decided that iodine should be considered for assessment of the risks associated with excess intake.
1.17 SACN agreed that, where appropriate, other expert committees would be consulted and asked to complete relevant risk assessments e.g. in the area of food safety advice to support their review. Therefore, the Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment (COT) was asked to consider whether exposure to excess iodine would pose a risk to maternal health, as part of this review.
1.18 In the environment, iodine is usually found in the form of iodate salts, or in the form of organo-iodide compounds produced by algae and bacteria. Iodine is essential in the human diet because it is required for the synthesis of the thyroid hormones tri-iodo- and tetra-iodothyronine (T3 and T4 which is also known as thyroxine). This takes place in the thyroid gland. The thyroid hormones help regulate metabolism and ensure that the heart, brain and other organs function in a healthy manner. They are also involved in brain development and bone growth especially in the fetus. The fetus is exposed to iodine via the placenta, and both maternal iodine deficiency and excess can have profound effects on both mother and offspring.
1.19 Excess iodine may lead to the occurrence of goitre in adults and children.
1.20 Goitre is a condition where a lump or swelling at the front of the neck caused by a swollen thyroid.
1.21 There are currently three health based guidance values (HGBV) set for iodine. Joint FAO/WHO Expert Committee on Food Additives (JECFA) established a Provisional Maximum Tolerable Daily Intake (PMTDI) of 17 μg/kg bw/day (equivalent to 1020 μg/day for a 60 kg adult) for iodine from all sources. The Expert Group on Vitamins and Minerals (EVM) set a guidance level for iodine of 15 μg/kg bw/day. The European Scientific Committee on Food (SCF) established a Upper Limit (UL) for total iodine intake of 600 µg/day.
1.22 Overall, the Committee concluded that there are no toxicological concerns at the levels of iodine exposure in the general population, however, high consumers of seaweed may be exposed to levels of iodine that could pose a toxicological risk to maternal health. Currently, available data are not sufficient to assess the applicability of the HBGVs to pregnant women, and there is a lack of exposure data in relation to pregnancy and lactation to enable a risk assessment to be performed. The full COT statement can be found at: Statement on the potential effects that excess iodine intake may have during preconception, pregnancy and lactation | Committee on Toxicity (food.gov.uk)
Statement on the effects of excess Vitamin A on maternal health
1.23 In 2019, SACN agreed to conduct a risk assessment on nutrition and maternal health focusing on maternal outcomes during pregnancy, childbirth and up to 24 months after delivery; this would include the effects of chemical contaminants and excess nutrients in the diet. The Committee on Toxicity was consulted, and decided that Vitamin A should be considered for assessment of the risks associated with excess intake.
1.24 Vitamin A (also known as retinol) is found in foods of animal origin (such as liver, paté and cod liver oil) and is also formed in the body when beta-carotene – the colouring matter in red and yellow, and leafy green vegetables – is broken down. The NHS lists significant food sources of vitamin A as cheese, eggs, oily fish, fortified low-fat spreads, milk, yoghurt and liver and liver products such as paté. Significant sources of beta-carotene include vegetables such as carrots, sweet potatoes, red peppers and spinach, and some fruit such as mango, papaya and apricots.
1.25 Retinol is converted, after it is eaten, into other chemical forms that are involved in several biological functions, such as the proper growth of the fetus in pregnancy (in a form called retinoic acid) and how the retina in the eye senses light (in a form called retinal). Most of the effects of vitamin A are caused by retinoic acid, which, among other things, influences bone development and secretion of hormones from the thyroid gland, and stimulates the immune system improving resistance to infections. Different chemical forms of vitamin A and synthetic substances that mimic it are also used as medicines, for example, to treat severe acne.
1.26 Although Vitamin A is vital to health and has many benefits, too much of it can cause health problems. A very high dose of vitamin A in the form of retinol can cause tiredness, joint pain, dry skin, headache, sickness, hair loss, drowsiness, liver and bone damage and sight problems. Vitamin A also accumulates in the liver and taking it over a long period of time can cause dry thickening of the skin, cracking of lips, damage to the eyes, skin reddening, hair loss, brittle bones, joint pain, lasting headache, increased pressure inside the skull and liver damage. Some, but not all, of these effects are reversible on reducing vitamin A intake.
1.27 Although it is broken down in the body to produce retinol, eating vegetables that are rich in beta-carotene, or consuming beta-carotene itself, does not result in adverse effects (except possibly high dose supplements in smokers) because less than one-third of beta-carotene from plant sources gets absorbed by the body.
1.28 Eating fat-rich food increases the absorption of vitamin A from the digestive system. The vitamin is carried on proteins in the blood to the liver, where it is stored and then distributed to the rest of the body to perform its functions. Vitamin A is excreted from the body largely in the urine, but as it accumulates in the liver, more is released in the bile, which may prevent the liver from being exposed to too much vitamin A
Effects of vitamin A on reproduction
1.29 Vitamin A is necessary for the proper functioning of the male and female reproductive systems, both inadequate and excessive amounts can harm the unborn fetus. The statement on vitamin A is concerned with the effects of excessive amounts of vitamin A (rather than inadequate amounts) and ill-effects from over- exposure. Excessive amounts of vitamin A can cause malformations to the fetus that include spina bifida (abnormal development of the spine), small or no eyes, harelip, cleft palate, absent or deformed ears, and deformities of limbs, kidneys, genitals, heart, thyroid gland and skeleton.
1.30 The UK Government recommends that, in order to avoid possible harm to the unborn child, pregnant women, or women thinking about having a baby or trying to conceive, should not consume liver or liver products such as paté, or supplements that contain vitamin A, including fish liver oil, unless they are advised to do so by a doctor. EFSA set a TUL for vitamin A of 3,000 µg per day for women of childbearing age, based on the risk of damage to the liver and to any unborn child. The UK Expert Committee on Vitamins and Minerals (EVM) considered that an intake greater that 1,500 µg per day was “inappropriate”, based on possible effects on bone. The World Health Organisation (WHO) recommends that vitamin A supplements should not be given to pregnant women except to prevent night blindness in places where vitamin A deficiency is a severe public health problem (which does not include the UK).
1.31 Taking food supplements, like fortified food products and vitamin pills, is the most common way for people, including pregnant women and those considering pregnancy, to be exposed to high doses of vitamin A. Scientific studies have surveyed the effects of supplements on development of the fetus in humans where women have taken higher dose supplements during pregnancy. Malformations have been seen, but as the number of women taking these supplements was low, the actual amount of vitamin A that causes deformities in humans remains uncertain.
1.32 Treatment of acne by taking tablets of the drug isotretinoin, a potent synthetic form of retinoic acid, is very effective but has raised concern as a possible cause of malformations when taken by pregnant women. Some countries, including Canada and the EU countries advise women against becoming pregnant while taking isotretinoin. But there are still a few women who become pregnant while taking this drug, putting the fetus at potential risk.
1.33 Treating acne with creams and ointments that contain forms of vitamin A and/or synthetic substances that mimic it, appears to pose a much lower level of risk to the unborn child than treatments given by mouth. However, since these preparations are also known to be able to produce the same adverse effects on the fetus as tablets, when given at a sufficiently high dose, their use is likewise not recommended during pregnancy.
1.34 Concerns have been raised about a link between isotretinoin use and an increased risk of depression and suicide. However, recent evidence suggests that having acne can itself cause depression and hence, if anything, treatment with vitamin A analogues can improve mental health. Nevertheless, as explained above, women who are pregnant or trying to conceive should avoid taking isotretinoin because of the possible risk to the fetus.
1.35 The effects of vitamin A may be affected by:
a. Other components in the diet, including vitamins D, K,C and folate, some fats and zinc,
b. Alcohol,
c. Medicines including antibiotics, treatments for fungal infections, drugs for epilepsy, and
d. Chemicals in the environment including biocidal shop antifouling paints (i.e. paints that discourage growth of marine organisms) and flame retardants, for example form furniture.
1.36 One way they can do this is by affecting the rate of breakdown of vitamin A and its active products.
1.37 Consuming large amounts of beta-carotene, for example by eating a lot of carrots daily, may lead to some skin yellowing and a fall in the levels of vitamin A in the liver but, unlike intake of pre-formed vitamin A, studies on animals have shown no ill-effects of beta-carotene on their offspring.
1.38 A study showed that high intake of beta-carotene supplements, as part of a clinical trial, unexpectedly increased the incidence of lung cancer and overall mortality in smokers. However, smoking itself can damage the fetus, regardless of any additional adverse effects caused by consumption of beta-carotene, so women are anyway strongly advised against smoking during pregnancy.
1.39 In parts of Africa and south-west Asia, there is more concern about vitamin A deficiency and the harmful effects this has upon the health of unborn children. In developed countries (like the UK, USA and those in Europe), however, the concern is more about excess intake, as many people regularly consume more than the recommended daily amount, and in some cases, more than EFSA’s tolerable upper limit.
1.40 EFSA has estimated that most European adults consume between 816 and 1,498 µg of retinol per day. The UK Government dietary advice, on the NHS.uk website recommends a daily vitamin A intake from food, for those aged 19 to 64, of 700 µg for men and 600 µg for women. Official estimates are that in the UK women between 16 and 49 years of age actually have an intake of between 760 and 2600 µg per day, and the small number who regularly eat liver and liver products such as paté may consume up to 3 times this amount. Supplements containing vitamin A in the form of retinol can add 300 – 906 µg per serving. Pregnant women and women thinking about having a baby are therefore specifically warned to avoid taking supplements containing vitamin A and not to eat liver and liver products to avoid potential harm to the unborn child, unless specifically advised to do so by their Doctor. No other food provides as much vitamin A on its own, although some fortified spreads and “health foods” may, in combination, provide more than the recommended limit.
1.41 Food supplements containing beta-carotene do not have warnings against their use by pregnant women and women thinking about having a baby because this nutrient is considered low risk.
1.42 There is still a lot of uncertainty about how much vitamin A is likely to cause deformities in unborn children, therefore the COT agreed that the current UK Government advice to pregnant women and those planning pregnancy – as set out on NHS.uk website – that they should limit their intake of vitamin A to reduce this risk, remains appropriate.
1.43 The full COT statement can be found here: Statement 04/22 Vitamin A in the maternal diet (food.gov.uk)
Position paper on bamboo composites in food contact materials
1.44 Risk assessment advice on biobased food contact materials (BBFCMs) has been increasingly requested from the Food Standards Agency (FSA), hence it was considered timely for the Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment (COT) to review the available toxicological information on BBFCMs.
1.45 The COT acknowledged the challenges and complexities associated with BBFCMs and highlighted several limitations and knowledge gaps on BBFCMs research and regulation. These included labelling, composition (including biodegradability), contamination and standardisation.
1.46 The COT undertook a more detailed review of the potential health risks of bamboo composites in Food Contact Materials (FCMs) due to the increased number of incidents reported of non-compliant bamboo composite items (e.g. coffee cups) being placed onto the European market.
1.47 Until December 2020, reports in relation to bamboo composite FCMs were predominantly related to misleading labelling on packaging and/or their advertisement, as well as incidences of formaldehyde/melamine migration levels exceeding legal limits. Since 2021, and due to the EU’s conclusion that bamboo is an unauthorised additive within plastic FCMs, reports received by the FSA have predominantly been of non-compliance of plastic-bamboo FCMs in the European market. This included the advertisement of products from UK businesses on EU facing markets. No action appeared to have been taken on that basis prior to this year.
1.48 In 2019, the EFSA panel on FCMs was asked by the European Commission to assess whether the authorisation of untreated wood flour and fibres (FCM no. 96) as an additive in plastic food contact materials was still in accordance with EC Regulation 1935/2004, and also to consider whether bamboo could be considered under the scope of this authorisation. EFSA concluded that wood and bamboo should be considered distinct and each material regarded on a case-by-case basis. In addition, the food safety authorities of Belgium, Luxembourg and the Netherlands (Benelux) published a joint letter calling for the market withdrawal of bamboo- melamine plastics (NVWA, 2021a). In April 2021, the EC recommended that Member States should take stringent action on bamboo composite FCMs and set out a coordinated control plan. The UK FSA is aware of the stance by the EC and of the individual Member States and is considering an appropriate course of action based on scientific evidence.
1.49 The COT previously assessed the reports by the German Federal Institute for Risk Assessment (BfR) and the Netherlands Food and Consumer Product Safety Authority (NVWA) and noted that the BfR applied their own tolerable daily intake (TDI) of 0.6 mg/kg/day for formaldehyde whereas the NVWA and EFSA used a lower TDI of 0.15 mg/kg/day (BfR 2020; NVWA 2021b; COT 2021c). Overall, the COT concluded that the exposure assessments were conservative but not necessarily worst-case. It was agreed that although the NVWA and BfR opinions took slightly different approaches, in general the same conclusions were reached. Based on the assessment of the BfR and NVWA reports the Committee concluded that the migration of formaldehyde and melamine from bamboo composite cups was a potential concern to human health (COT 2021c).
1.50 Due to insufficient UK data, the COT was unable to make recommendations on bamboo bio-composites FCMs. A UK study assessing the risks associated with bamboo composites and other biobased food contact materials is currently underway. The study aims to address migration levels of formaldehyde and melamine, and also the potential presence of other chemicals, such as heavy metals and pesticide residues. Data from this study is expected to be available in March 2022. Once, UK data is available, a full risk assessment will be undertaken.
1.51 The full COT statement can be found here: COT Position Paper Bamboo Composites
COT statement on the potential risks from cadmium in the maternal diet
1.52 In 2019 the Scientific Advisory Committee on Nutrition (SACN) agreed to conduct a risk assessment on nutrition and maternal health focusing on maternal outcomes during pregnancy, childbirth and up to 24 months after delivery; this would include the effects of chemical contaminants and excess nutrients in the diet. The Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment (COT) were asked to review the risks of toxicity from chemicals in the maternal diet.
1.53 Cadmium is a heavy metal found widely in the environment, coming from both natural sources, such as volcanic activity, and human activities, such as the smelting of metals. Cadmium in the soil, water and air enters the human food chain through being taken up by crops, which are consumed by food animals. Once in the body, this metal accumulates over many years, where it may cause damage to the kidneys and loss of bone tissue. It can also cause cancer.
1.54 Those of childbearing age (16-49 years) can be exposed to cadmium from food, drinking water, air, dust and ingested soil. Smoking is the main non-dietary source of exposure of cadmium and can lead to a similar internal exposure as the obtained from the diet.
1.55 In 2009, the EFSA CONTAM panel established a tolerable weekly intake (TWI) based on the adverse effect on the kidneys, to determine the level of exposure of people below which there would be no cause for concern. The TWI is defined as the amount of cadmium that can be taken in by a person every week throughout their lifetime without causing adverse effects on health. This value was very low at 2.5 micrograms (millionths of a gram) per kilogram body weight. The COT had previously concluded that the EFSA TWI for cadmium was an acceptable value to use for risk assessment.
1.56 The COT concluded that the levels of cadmium in water, soil and dust only contribute a small amount of exposure and overall, cadmium in the maternal diet does not appear to be a health concern.
1.57 The COT highlighted that the consumption data used for the exposure assessment was for women of childbearing age and therefore may not be fully representative of the maternal diet, leading to an under/overestimation of the actual exposure. The COT also noted that women who give up smoking while pregnant will still carry a higher body burden of cadmium than those who had never smoked.
1.58 The full COT statement can be found at: Cadmium in the Maternal Diet - Introduction | Committee on Toxicity (food.gov.uk)
Statement on the potential effects of excess vitamin D intake during preconception, pregnancy and lactation
1.59 In 2006, the European Commission established a minimum vitamin D content in infant- and follow-on formulae of 1 µg per 100 kcal (Directive 2006/141/EC). Subsequently in 2016, in Commission Delegated Regulation 2016/127, this was doubled to 2 µg per 100 kcal. This new regulation became applicable in Great Britain from the 1st of January 2021.
1.60 In order to inform discussion across the four nations on whether existing advice around vitamin D supplements remains appropriate or needed updating in light of the increase in the minimum vitamin D content of infant- and follow-on formulae, the FSA conducted an exposure assessment to determine whether this increase could result in infants (0-12 month-olds) and young children (1-4 year-olds) exceeding their tolerable upper levels (TULs) .
1.61 A draft statement was prepared which provides an exposure assessment for infants and young children, regarding their vitamin D intake from infant formulae products, vitamin D supplements, and other dietary sources (including breast milk), and comparison to the relevant EFSA TULs.
1.62 The Committee concluded that the new minimum vitamin D content in infant formulae did not lead to excessive vitamin D exposure in infants or young children, as minor exceedances of their respective TULs occurred only when, in combination with other sources such as the recommended supplements, the quantities of infant formula consumed reached 1000 ml. Current NHS guidance is that supplementation is not needed if more than 500 ml infant formula is being consumed. The Committee agreed with the recently revised TUL of 35 μg/person/day for 6-12 month-olds, and also that the exposure assessment indicated that the current guidance did not give rise to any toxicological concerns.
1.63 The full COT Statement can be found here: Vitamin D in infant formula statement
Potential approaches to address unintentional mixture risks for future UK REACH assessments
1.64 In September 2020, the UK Chemicals Delivery Board had agreed that the Environment Agency should prepare a report on whether the use of a mixture assessment factor (MAF) is a useful approach to address the potential risks arising from unintentional (coincidental) mixtures of chemicals under the UK REACH (Registration, Evaluation, Authorisation, and Restriction of Chemicals) Regulation. Risks from intentional mixtures are already covered under the current regulatory system. This approach was also being considered by the European Union under EU REACH. Subsequently, the UK Health Security Agency (UKHSA) had agreed that they would work with the Environment Agency to prepare a joint report.
1.65 The COT considered the draft version of the joint EA/UKHSA report on this topic in March and May 2022 to review and comment on the human health aspects prior to finalisation of the report.
1.66 A number of recommendations and comments were made by the COT in March, which were addressed in the version presented in May. The COT recognised that while there were publications hypothesising that environmental mixtures of chemicals might have an additive effect, the evidence available suggested that any potential effects were almost always driven by exposure to a small number of chemicals, even when there were a large number of substances in the mixtures considered. Similar findings had also been reported in three EFSA retrospective cumulative risk assessments of dietary exposure to mixtures of pesticide residues. The Committee noted the lack of research available to address the question of whether there was dose addition for chemicals present in a mixture at concentrations below their health-based guidance values (HBGVs). In many studies, whilst findings at effect levels were consistent with dose addition, they were also consistent with response addition (independent action). Hence, whilst dose addition might be a reasonable default at exposure levels above health-based guidance values, it was highly questionable whether this was the case at lower levels and consequently whether a MAF was needed.
1.67 Overall, the COT agreed with the conclusions of the report and in particular that there was strong scientific evidence within the report to support not adopting the use of a MAF in human health risk assessments.
1.68 The EA/UKHSA report “Evaluation of the potential approaches to risk assessment of unintentional chemical mixtures for future UK REACH assessments” was published following comments from COT and Defra’s Hazardous Substances Advisory Committee (HSAC) and is available from: Evaluation of the potential approaches to risk assessment of unintentional chemical mixtures for future UK REACH assessments - GOV.UK (www.gov.uk)
1.69 Contribution for update paper (2022 paper to give an indication on the level of information is available from: Update on Advice (food.gov.uk)
Potential approaches to address unintentional mixture risks for future UK REACH assessments
1.70 The EA/UKHSA report “Evaluation of the potential approaches to risk assessment of unintentional chemical mixtures for future UK REACH assessments” was published following comments from COT and Defra’s Hazardous Substances Advisory Committee (HSAC) in August 2022, and is available from: Evaluation of the potential approaches to risk assessment of unintentional chemical mixtures for future UK REACH assessments - GOV.UK (www.gov.uk)
1.71 In December 2022, a stakeholder workshop was hosted by Defra to discuss options for addressing unintentional mixtures under UK REACH. The report and the outputs from this workshop will be considered by Defra to inform the development of policy options.
Review of potential risks of Aflatoxin in foodstuffs at the new proposed Codex Alimentarius maximum levels - RESERVED Business
1.72 The FSA asked the Committee to review the toxicity of aflatoxins in certain foodstuffs. This item is currently reserved as it relates to developing policy.
Review of potential risk of Ochratoxin A in spices at the proposed Codex Alimentarius Levels (RESERVED Business)
1.73 The FSA asked the Committee to review the toxicity of Ochratoxin A in spices. This item is currently reserved as it relates to developing policy.
Discussion paper on the request for assessment of a coating in canned food packaging materials
1.74 Members discussed the information provided to the Committee on a can coating as well as the assessment and discussions of the Joint Expert Group on Food Contact Materials (FCM JEG) and sister Committee on Mutagenicity (COM). The work is ongoing, but a final assessment is expected in spring 2023. This item is reserved as the data are commercially confidential.
Committee Procedures
Response to EFSA consultation on BPA
1.75 In December 2021, the EFSA Panel on Food Contact Materials, Enzymes and Processing Aids (CEP) published a draft opinion re-evaluating the health risks arising from the presence of bisphenol A (BPA) in food. The panel proposed a significant reduction to the current temporary Tolerable Daily Intake (TDI) of 4 µg/kg body weight (bw) to 0.04 ng/kg bw. This reduction would mean that both mean and high level consumers for all age groups would exceed the new TDI by 2-4 orders of magnitude.
1.76 Due to the size and complexity of the draft opinion, the COT held an extraordinary meeting to discuss it, before feedback was then provided to EFSA as part of their consultation process. The Committee considered the Health Outcome Category (HOC)/cluster approach used by the EFSA CEP panel to conduct the evaluation comparing it to the approach taken by the COT and COC Synthesis and Integration of Epidemiological and Toxicological Evidence subgroup (SETE). The Committee also discussed the benchmark dose modelling used by EFSA including the uncertainty analysis and derivation of the Health Based Guidance Value (HBGV). The Committee then considered the toxicokinetics along with the specific endpoints of immunotoxicity, reproductive and developmental toxicity, neurotoxicity and developmental neurotoxicity, genotoxicity, and other minor endpoints; the approach to epidemiology, metabolic effects, cardiotoxicity, and carcinogenicity.
1.77 The comments agreed by the Committee were submitted to EFSA as part of their public consultation process. The final EFSA opinion is expected to be published towards the end of 2022.
EFSA Copper Opinion
1.78 The European Food Safety Authority Scientific Committee were asked by the European Commission to review the existing scientific evidence and all new relevant studies with the aims:
- to provide a scientific opinion on an ADI for copper which can be used as a reference value for copper containing regulated products.
- to take into account all sources of exposure and integrate different approaches and scenarios, to perform a new estimation of the overall copper intake which includes contributions from all major sources of exposure.
1.79 The Committee considered the approach used by the EFSA Scientific Committee to establish the Acceptable Daily Intake (ADI) for copper and the studies used by the Scientific Committee to reach their conclusions. The pivotal studies used by EFSA to determine the HBGV were Turnlund et al., (2005) and Harvey et al., (2003) which examined copper homeostasis. The Committee discussed these studies and highlighted that there was a limited number of participants which were all male that could have an impact on the reliability of the HBGV. However, it was noted that the homeostatic response would not vary in relation to age, sex or pregnancy.
1.80 In conclusion, the Committee agreed that EFSA’s proposed new HBGV of 5 mg/kg bw per day and the harmonised approach used to establish it were acceptable.
1.81 The comments agreed by the Committee were submitted to EFSA as part of their public consultation process.
Draft FSA/HSE/VMD report on approaches to chronic dietary exposure assessment for chemicals in food
1.82 The COT was asked to comment on a report drafted by FSA, the Health and Safety Executive (HSE) and the Veterinary Medicines Directorate (VMD) on approaches to chronic dietary exposure assessment for chemicals in food. The draft report was also being taken to the Expert Committee on Pesticides (ECP) and the Expert Committee on Pesticide Residues in Food (PRiF) for comment before being finalised.
1.83 The work had been undertaken because there were differences in the current approaches to chronic dietary exposure assessments undertaken by the HSE for pesticides, VMD for veterinary medicines and FSA for chemical contaminants and other chemicals in food. Furthermore, there were differences in how these assessments were conducted internationally for pesticides and emerging differences for veterinary medicines. In addition, following exit from the EU, it was timely for UK regulators to consider the approaches they might wish to take in the future.
1.84 The draft report discussed the principles of dietary exposure assessments and described the current approaches to chronic dietary exposure assessments being taken by the FSA and for pesticides and veterinary medicines. It discussed the current differences in approach and the reasons for them, uncertainties in exposure assessments, considered the possibilities for common approaches to be taken in the future and the approaches to substances with multiple uses (e.g. as both pesticides and veterinary medicines). It also included some considerations on cumulative and aggregate exposure assessment and referred to the recent considerations of less than lifetime and variable exposure over a lifetime by the COT and COC.
1.85 The draft report made a number of recommendations. These included increasing collaboration between FSA, HSE and VMD on topics such as exposure assessments for substances with multiple uses, the setting of common Maximum Residue Levels (MRLs) and Health Based Guidance Values (HBGVs), and on methodologies for cumulative risk assessments; continuing international collaborations; periodically reviewing exposure assessment methodologies for fitness for purpose and considering their uncertainties; and having up-to-date comprehensive food consumption data, which are contained within a central database to which staff from each of the departments/agencies have access and training on their use.
1.86 The COT advised that the recommendations be separated out from the conclusions. The FSA’s approach was noted to be usually closer to actual consumer exposures compared to regulatory approaches for approvals of pesticides and veterinary medicines. If joint exposure assessments were to be performed it would need to be agreed what degree of conservatism there should be. The COT supported the desire for more information on cumulative and aggregate exposures but the methods were not fully developed yet and there were still improvements that could and should be made to exposure assessments for single substances first. Probabilistic modelling was included in the report as a high tier model but that was not being conducted to much extent at the moment, though the software was available and it could be used more. There was also agreement with the recommendation of a central database for food consumption data.
1.87 The COT considered that it was a good idea to conduct exposure assessments more consistently across chemical areas; however, it was noted that for applicants there was also the international consideration and to them it would be preferable for there to not be too many differences in the approaches used between regions internationally, e.g. between the UK and Europe.
1.88 The COT noted that EFSA had taken one approach to the cumulative risk assessments of pesticides and a different approach to other chemicals. While they had produced guidance it was not clear whether they were currently routinely undertaking cumulative risk assessments for chemicals other than pesticides. Where such cumulative risk assessments had been performed, a constrained approach tended to have been taken, for example, grouping chemicals in the same regulatory area that have similar structures. At present, there did not appear to be have been any move to conder, for example, all chemicals across all sectors that cause hepatic steatosis as a single group, for regulatory purposes. The COT suggested that the report should recognise the difficulties as well as the possibilities of performing combined exposure assessments across different regulatory areas.
1.89 The COT observed differences in the age ranges being used currently to define infants and children, asked for justification for the use of the 97.5th percentile to represent high consumers to be included in the report, and discussed the extent to which the National Diet and Nutrition Survey (NDNS) adequately covered ethnic groups and groups such as vegans. The NDNS reflected the whole population but focused studies would be needed to reflect the consumption patterns of groups that comprise only small percentages of the entire population, to ensure their adequate statistical characterisation.
1.90 It was noted that exposure assessors are constrained by the data that they can obtain. For example, JECFA and JMPR do not have access to consumption data with the level of granularity that the FSA has, and hence would have considerable difficulties in performing probabilistic modelling.
1.91 The draft report would be revised and published after the ECP and PRiF had also commented.
Statement on the EFSA Opinion on the risks to human health related to the presence of perfluoroalkyl substances in food
1.92 The European Food Safety Authority (EFSA) was asked, by the European Commission, to prepare an Opinion on the risks to human health related to the presence of perfluoroalkylated substances (PFASs) in food, and to consider existing hazard assessments and available occurrence data. The statement was published in September 2020.
1.93 The Committee on Toxicity of Chemicals in Food, Consumer products and the Environment (COT) have reviewed the “EFSA Opinion Risk to human health related to the presence of perfluoroalkyl substances in food” (2020) alongside UK exposure data to assess the potential risks to the UK population from PFASs (predominantly through exposure via the diet).
1.94 Per- and polyfluoroalkyl substances (PFASs) with a minimum of six carbons in their backbone, are a class of over 12,000 fluorinated substances (US EPA CompTox Dashboard 2022). They have been produced since the 1940s and are, or have been, used in a broad range of consumer products and industrial applications (Glüge et al., 2020). Their structure enhances their utility in a variety of applications including the production of water- and oil-resistant clothing, electronics, non-stick cookware, carpets, and food packaging materials.
1.95 Many PFASs are environmentally long-lived and individuals are exposed to them through all environmental sources, i.e. drinking water, air, dust, and the diet and through the placenta and breastfeeding for developing offspring (Sunderland et al., 2019).
1.96 The tolerable weekly intake (TWI) was established by EFSA based on epidemiological studies of an effect on the immune system, as this was considered, by the EFSA CONTAM Panel, to be the critical effect. Two studies on this (Abraham et al., 2020 and Grandjean et al., 2012) were considered by EFSA as suitable for hazard characterisation. One of these studies, Abraham et al. (2020), was amenable to dose-response modelling (i.e. analysis of the response of an organism, as a function of exposure (or doses) to a chemical after a certain exposure time); which resulted in a benchmark dose limit value (BMDL10) for blood serum of 17.5 ng/mL for the sum of the four main PFASs present. This value was then used as the reference point to calculate the corresponding tolerable daily intake for a mother, to protect their offspring, considered the most sensitive population, which was 0.63 ng/kg body weight (bw) per day. This was then converted to a weekly value, because of the long persistence of PFASs in the body, the TWI, of 4.4 ng/kg bw per week for the sum of the four PFASs PFOS, PFOA, PFHxS and PFNA, for use as the health-based guidance value.
1.97 The COT agreed that, on the basis of the information reviewed by EFSA, qualitatively the appropriate health endpoint had been selected but quantitatively, questioned the calculations. Overall, there were some reservations about the choice of the critical study (Abraham et al., 2020) and the specific effect that was selected. However, the COT agreed that the critical study was the best available; and, in the absence of more appropriate studies, its use was understandable. Therefore, it was not unreasonable that this study was selected.
1.98 The COT had significant reservations about the dose-response model used, including the modelling approach, and the TWI which had been established, due to the uncertainties and the caveats involved.
1.99 The COT agreed that the use of the sum of the four PFASs was acceptable as a first approximation for exposures of PFASs but had reservations about the calculations due to the uncertainties.
1.100 The diet is the predominant route of exposure to PFASs, however, other possible sources of exposure include dust by ingestion and indoor air by inhalation, and these exposures have been considered. There may also be some exposure via the skin, however these have not been calculated.
1.101 The values for the BMDL and TWI were low and there was a lot of uncertainty surrounding the data used by EFSA.
1.102 Estimated breast milk exposures for UK infants all exceed the TWI of 4.4 ng/kg bw per week. However, EFSA cautions that “the higher exposure of breastfed infants is taken into account in the derivation of the TWI (i.e. it is assumed that those later exposed have already received this exposure) and the intake by infants should therefore not be compared with this TWI”.
1.103 Blood serum level modelling of the four PFASs indicates that the lower bound estimates of exposure (assuming that levels below detection are zero) is a more accurate prediction of the exposure than the upper bound estimates (assuming that levels below detection are present at that level), which would lead to a much higher exceedance of the critical blood serum levels. Lower bound mean estimated dietary exposures for adolescents, adults, the elderly and the very elderly approximate the TWI, that for other children is approximately twice the TWI, and for infants and toddlers are several times the TWI.
1.104 Estimated exposures from household dust at average median PFASs concentrations for all UK populations, for individual PFASs, are below the TWI. For exposures estimated from average maximum PFASs concentrations in household dust the TWI is exceeded for PFOS, PFOA and PFHxS by infants, toddlers and children.
1.105 The EFSA CONTAM Panel, in their evaluation of PFASs, assessed exposure both to individual compounds and using a mixtures approach (i.e. a probabilistic model for representing the presence of subpopulations within an overall population, without requiring that an observed data set should identify the sub-population to which an individual observation belongs) for the sum of four PFASs: PFOS, PFOA, PFHxS and PFNA. All exposure estimates were compared to the TWI of 4.4 ng/kg bw per week. The CONTAM Panel considered that the impact of the uncertainties on the risk assessment for the sum of PFOA, PFNA, PFHxS and PFOS is high.
1.106 The exceedances of the TWI at lower bound exposure estimates indicate a potential health concern.
1.107 Whilst the COT is unable to suggest an alternative TWI at this time due to the lack of data, there are strong caveats when comparing the exposure estimates with the TWI established by EFSA. There is considerable uncertainty as to the appropriateness of the derivation of the TWI and of the biological significance of the response on which it is based.
1.108 The COT suggested that in future reviews it could use the averages for exposures for the four PFASs added together to provide a reasonable estimation of combined PFASs exposure for comparison to the TWI.
1.109 The full statement can be found at: Statement on the EFSA Opinion on the risks to human health related to the presence of perfluoroalkyl substances in food
Nitrosamines
1.110 EFSA published a draft Scientific Opinion on the human health risks related to the presence of N-nitrosamines (N-NAs) in food for consultation October 2022. The COT were asked to provide comments on this draft.
1.111 Nitrosamines are the reaction products formed from nitrosating agents, such as nitrites or nitrogen oxides, and amino-based substances, such as secondary amines. They may be formed in a variety of foods (e.g., cured meat products, processed fish, beer and other alcoholic and non-alcoholic beverages, cheese, soy sauce, oils and processed vegetables) under processing conditions in the presence of these reactants.
1.112 It was considered that the draft Opinion provided a good summary in terms of ADME and genotoxicity data. It was commented that the main issues open to question were the method of benchmark dose (BMD) analysis and how compounds were aggregated (grouped).
1.113 Positive feedback was provided on the draft Opinion, which Members considered to be a comprehensive review of the topic. The comments agreed by the Committee were submitted to EFSA as part of their public consultation process.
On going work
Lead in the Maternal Diet
1.114 As part of the work on the maternal diet, the COT was asked to consider the potential effects that excess lead intake may have in the maternal diet.
1.115 Lead is a heavy metal that occurs naturally in the Earth’s crust, chiefly as lead sulphide (PbS). Lead is ubiquitous in the environment and is thus present in the diet of the general population, including women of childbearing age. Despite this, dietary levels have fallen since the phasing out of lead in petrol, plumbing and paints.
1.116 Potential risks from maternal exposures to lead were characterised by margins of exposure (MOEs), calculated as the ratio of the benchmark dose level (BMDL) to estimated exposures from diet, soil and air. A BMDL01 has been set for the reduced development of intellectual function in offspring. Specifically, a dietary exposure of 0.5 µg/kg bw/day was associated with a 1% change in full scale IQ score (EFSA 2010).
1.117 As the BMDL was for a small effect, it is likely to be conservative and protective for all other adverse effects of lead in all populations, including the mother. EFSA concluded that a margin of exposure of 10 or greater should be sufficient to ensure that there was no appreciable risk of a clinically significant effect on IQ. At lower MOEs, but greater than 1, the risk is likely to be low, but not such that it could be dismissed as of no potential concern (EFSA, 2010). In 2013, the COT added that an MOE of >1 can be taken to imply that at most, any risk is likely to be small. MOEs <1 do not necessarily indicate a concern, but scientific uncertainties mean that a material risk cannot be ruled out.
1.118 Lead was initially discussed at the February 2022 COT meeting. The Committee considered issues such as exposure to food, drink and air. It was determined that other sources of exposure should also be considered such as soil and dust due to the ubiquitous nature of lead in the environment; this was discussed at the May 2022 meeting.
1.119 It was concluded that while MOE values were ≥1 for all exposure scenarios, lead toxicity would depend on total exposure from all sources, therefore an aggregate exposure to determine an overall likely level of risk was appropriate.
1.120 A statement setting out the views of the Committee on will be published in 2023.
Potential risk to human health of turmeric and curcumin supplements
1.121 The FSA has been monitoring incidents related to consumption of raw and powdered turmeric and its supplements. In light of these incidents and due to the uncertainties surrounding the composition and possible contamination of these commodities, the COT was asked to comment on the risk to human health from turmeric and curcuminoids in their various forms which include supplements.
1.122 To aid this discussion a survey of 30 products was undertaken by Fera Science Ltd in 2021. All samples were analysed for the curcuminoids: curcumin, bisdemethoxycurcumin (BDMC) and demethoxycurcumin (DMC) as well as the black pepper derived alkaloid, piperine; and a comprehensive analysis of 69 trace elements which included the heavy metals lead (Pb), mercury (Hg), arsenic (As) and cadmium (Cd). A further 70 turmeric products were analysed for Pb in 2022.
1.123 After reviewing the results of the survey, the Committee concluded that Pb contamination of turmeric products was not likely to be the reason for hepatotoxicity incidents.
1.124 The COT further concluded that substantial exceedances of the dietary ADI, which may occur from consumption of currently available supplements, represented a potential health risk to humans, especially if other medicines are being taken concomitantly and for individuals with altered hepato-biliary function. Furthermore, in rare individuals, consumption of turmeric at the levels found in supplements, even at low concentrations where exposure was below the ADI) may pose a risk of adverse effects to the liver, due to idiosyncratic responses. This possibility of an unexpected idiosyncratic response should be considered when providing guidance on the use of such supplements.
1.125 A final COT statement is due to be published early 2023.
Oral Nicotine pouches
1.126 The COT was requested by the Tobacco team in the Office of Health Improvement and Disparities at DHSC (OHID) to consider the toxicological risk for nicotine-free or nicotine pouches.
1.127 In 2022, the COT discussed updated paper providing publicly available data on the ingredients in these products along with an assessment of the oral bioavailability of nicotine. Following this, a first draft statement was presented on the bioavailability of nicotine from the use of oral nicotine pouches and assessment of the potential toxicological risk to users.
1.128 The COT agreed with the overall conclusions presented in the statement; several minor comments on the general structure and content of the draft statement would be addressed by correspondence. It is anticipated that the statement would be finalised in 2023.
Risk assessment of potential constituents and contaminants in cow’s milk
1.129 Plant-based drinks have become increasingly popular in the United Kingdom (UK) both for individuals with an allergy to cows’ milk or lactose intolerance and those who wish to avoid dairy products for other ethical or cultural reasons.
1.130 Current UK Government advice regarding the use of plant-based drinks for infants and young children is that unsweetened calcium-fortified plant-based drinks, such as soya, oat and almond drinks, can be given to children from the age of 12 months as part of a healthy balanced diet; rice drinks should not be given due to the levels of arsenic in these products (NHS, 2018).
1.131 The Committee agreed during their meeting of July 2021 the main comparator for plant-based drinks should be cow’s milk and that a discussion paper should be produced looking at the potential chemical risks in the consumption of this for the population group of interest, children aged 6 months to 5 years.
1.132 Over the course of 2021 two discussion papers were produced reviewing a range of compounds found in cow’s milk. The compounds covered included veterinary medicines, pesticides, nitrate and nitrite, bisphenol A, phthalates, dioxins and dioxin-like biphenyls, non-dioxin-like polychlorinated biphenyls, polycyclic aromatic hydrocarbons and isoflavones. A selection of heavy metals, iodine, chlorate and perchlorate, mycotoxins, naturally occurring oestrogens in cows’ milk, insulin like growth factor, per- and polyfluoroalkyl substances, brominated flame retardants and microplastics were also considered.
1.133 Following this work, over the course of 2022 two draft statements were drafted and presented for the COT regarding cow’s milk. Within these draft statements, iodine and aflatoxin M1 were indicated as being of low concern and risk relating to isoflavones was considered uncertain due to a lack of health based guidance values for young children.
1.134 A final statement will be published in 2023.
Microplastics – exposure via the inhalation route
1.135 As part of horizon scanning exercise, the COT identified the potential risks from microplastics as a topic it should consider to inform Food Standards Agency (FSA) discussions on this. Since then, several discussion papers have been presented to the COT and in 2021, an overarching statement on the potential risks from exposure to microplastics was published (COT Statement 2021/02). This provided a high-level overview of the current state of knowledge, data gaps and research requirements with regards to this topic. This was followed by a sub- statement which considered the potential effects of oral exposure to microplastics in more detail.
1.136 As there is evidence for the presence of plastic particles in both indoor and outdoor air inhalation is a possible route of exposure. The Committee is therefore discussing a sub-statement on inhalation exposure to microplastics to provide more detailed, supplementary information on this topic. This will be finalised in 2023.
Chitin and chitosan in food packaging materials
1.137 The COT is currently assessing whether there are any potential health risks posed by bio-based food contact materials (BBFCMs). One of the first materials to be reviewed was food packaging materials which contain chitin or chitosan.
1.138 Chitin and chitosan can be derived from fungi, insects, or shellfish. As there are potential concerns for allergic individuals, the Committee agreed that during its manufacture, the protein content in the specification of chitosan needs to be considered.
1.139 The Committee noted that due to a scarcity of relevant data in the scientific literature, it is not currently possible to undertake a reliable exposure assessment due to the uncertainties involved.
1.140 The COT further noted that whilst the risk of allergenicity from these BBFCMs appears to be low, it would be useful to have an indication or estimation of total exposures to allergenic proteins from BBFCMs, for example the upper bound levels of ingestion, or range of amounts of BBFCMs in contact with different foods. A position paper on chitosan will be prepared in 2023.
Statement paper on the guidance levels for the fortificants in the bread and flour regulations
1.141 The Bread and Flour regulation (BFR) stipulates the levels of calcium carbonate, iron, thiamin (also known as vitamin B1) and nicotinic acid that must be present in flour. In 2022, the Department for Environment, Food and Rural Affairs (Defra) held a consultation on the BFR 1998 review and asked whether the consultees agreed with the proposal to raise the minimum levels of calcium carbonate, iron and niacin added in non-wholemeal wheat flour to 15% of the nutrient reference values (NRV) supplied by 100g of flour as stated in point 1 of Part A of Annex XIII of regulation EC No. 1169/2011. NRVs are established guidelines for the recommended daily energy and nutrient consumption. The minimum amount of thiamin required to be present in non-wholemeal wheat flour will remain the same at 19% of the NRV.
1.142 The COT were asked by DHSC to provide a risk assessment on the dietary exposure of calcium carbonate, iron, nicotinic acid and thiamin at the current and proposed fortification levels to identify if there were any potential adverse health effects. The Committee considered the the potential exposures from the proposed changes and the adverse effects associated with high calcium, iron and thiamine intakes.
1.143 Acute and chronic intakes for all minerals (calcium, iron niacin and thamin) at the current and proposed fortification levels in food did not exceed the levels considered to be acutely toxic and were not considered to be a health concern.
1.144 Intakes of calcium from supplements alone did not exceed the guidance level. However, daily intakes of iron, niacin and thamin from supplements alone may result in exceedance of Health Based Guidance Values when higher dosage supplements are consumed. However, not all of the population consume supplements. Therefore, any potential health risks will only occur in individuals who consume high dosage iron, niacin and thiamin supplements.
1.145 Intakes of calcium from both food and supplements would not result in exceedance of HBGVs for calcium. However, intakes of iron, niacin and thamin from food and supplements combined could lead to these being exceeded. Given, that exceedance occurs from supplement consumption alone, the exceedances of iron, niacin and thiamin here would only be of toxicological concern to individuals that also consume high dosage of iron, niacin and thiamin through supplements.
1.146 Overall, the COT concluded that the proposed increased in the fortification level of calcium, iron and niacin in non-wholemeal flour would not result in any excess risk. However, there would be a possible exceedance in individuals that consume supplemental iron, niacin and thiamin alongside food containing and/or fortified with these minerals.
1.147 A final statement will be published in 2023.
Ginger in the maternal diet
1.148 As part of the current programme of work on the maternal diet, the Committee considered the use of herbal dietary supplements during pregnancy. These were supplements that were not officially recommended by the relevant authorities, but which were promoted by anecdotal evidence and unofficial sources as having various purported benefits. Ginger was identified as one of the supplements that should be considered in more detail.
1.149 Ginger (Zingiber officinale) is a flowering tropical plant originating in Southeast Asia and grown in warm climates including China, India, Africa and the Caribbean. The rhizome (underground stem) of the ginger plant is commonly used as a spice and flavouring in many countries around the world and is increasingly growing in popularity as a natural remedy due to its purported immune system-boosting properties and also for motion sickness and post-operative nausea and vomiting.
1.150 The COT have previously reviewed the potential effects of ginger and in particular, the use of ginger supplements during pregnancy and lactation, reviewing the available data on toxicity to the mother, effects on the development of the fetus or embryo, and possible interactions with medicines. In 2022, the Committee worked on a statement setting out their views. The statement is being revised to include information on the National Institute for Health and Care Excellence (NICE) and the European Medicines Agency (EMA) guidelines available on the on the use of ginger for nausea in pregnancy. And clarification on the exposure to ginger in the form of concentrated drinks and shots.
1.151 Further, the weight of evidence on spontaneous abortion as an outcome should be considered, along with the probability of this effect.
1.152 The statement will be finalised by the COT in 2023.
The potential risks from ergot alkaloids in the maternal diet
1.153 As part of the ongoing programme of work on the maternal diet, the Committee were asked whether exposure to ergot alkaloids (EAs) would pose a risk to maternal health.
1.154 Ergot alkaloids (EA) are secondary metabolites produced by the fungi families Clavicipitaceae and Trichocomaceae, with Claviceps purpurea being the most widespread Clavicepsspecies in Europe. Based on their occurrence and the available toxicological data the European Food Safety Authority (EFSA) considered six EAs in their risk assessment in 2005, namely: ergotamine, ergocornine, α- ergocryptine, ergosine, ergocristine (peptide ergot alkaloids) and ergometrine (a lysergic acid amide). EFSA further included both forms (-ine and inine) in their assessment, while the -inine forms are considered biologically inactive interconversion occurs under various conditions (EFSA, 2005, Tasker and Wipf, 2021). Bromocriptine is synthetic ergoline derivate and it is used in the treatment of Parkinson’s disease and pituitary tumours (Herdman et all., 2001).
1.155 The EA were discussed at July 2022 COT meeting. The Committee considered information on toxicology, metabolism and dietary exposure presented in the paper and raised a number of questions along with suggestions for data that should be considered. However, overall, Members considered that EAs would not have adverse effects on maternal health at likely levels of exposure. A statement will be prepared by the COT in 2023.
Raspberry Leaf tea in the maternal diet
1.156 As part of the current programme of work on the maternal diet, the Committee considered the use of herbal dietary supplements during pregnancy. These were supplements that were not officially recommended by the relevant authorities, but which were promoted by anecdotal evidence and unofficial sources as having various purported benefits. Raspberry leaf tea was identified as one of the supplements that should be considered in more detail.
1.157 Raspberry leaf was most commonly taken during pregnancy for its purported effects in stimulating and facilitating labour and in shortening its duration.
1.158 Members considered that it was not possible currently to derive a point of departure to be used in the risk assessment of raspberry leaf use during pregnancy, based on the data presented. There were numerous reasons for this.
1.159 It was agreed that a draft statement would be prepared in 2023 specifically cross-referencing the COT’s previous work on some of the components of raspberry leaf, such as polyphenols.
Green tea catechins
1.160 The COT had been asked by the FSA to evaluate green tea catechins and the associated probable idiosyncratic hepatotoxicity. This was following a request from the Nutrition Labelling Composition and Standards (NLCS) Common Framework, on behalf of the UK to evaluate whether the conclusions of the 2018 EFSA opinion on the safety of green tea catechins were still applicable considering any new scientific data that may have become available since its adoption. This would enable the NLCS to consider the next steps for the risk management of these compounds.
1.161 The 2018 EFSA Opinion concluded that catechins (principally - epigallocatechin-3-gallate (EGCG), from infusions or in reconstituted drinks are generally considered safe. However, rare cases of liver injury have been reported after consumption of green tea infusions, most probably due to an idiosyncratic reaction. Based on the available data on the potential adverse effects of green tea catechins on the liver, there is evidence from interventional clinical trials that intake of doses equal to or above 800 mg EGCG/day taken as a food supplement has been shown to induce a statistically significant increase of serum transaminases in treated subjects compared to control.
1.162 A statement on green tea catechins will be published in 2023.
How the Committees evaluate the relevance and reliability of data when assessing a chemical of concern
1.163 The COT, COC and COM have continued to develop the joint non-technical statement on how the Committees evaluate the relevance and reliability of data when assessing a chemical of concern in 2022. An updated version was presented to the COT in July. Further revisions are expected to be considered by correspondence across all three Committees in 2023.
An update of the COT position on aircraft cabin air
1.164 In 2007, the Committee on Toxicity (COT) published a statement on aircraft cabin air, having been asked by the Department for Transport (DfT) to undertake an independent scientific review of data submitted by the British Airline Pilots Association (BALPA) relating to organophosphate (OP) compounds, the cabin air environment, ill-health in aircraft crews and the possible relationship to smoke/fume events in aircraft, due to concerns about the possible effects on aircrew health of oil/hydraulic fluid smoke/fume contamination incidents in commercial aircraft (COT, 2007).
1.165 In 2013, DfT asked the COT to undertake an independent scientific review of the results of DfT-funded aircraft cabin environment research commissioned in response to recommendations made by COT in 2007, after which the COT issued a position statement on cabin air (COT, 2013).
1.166 The COT has now been asked by DfT to investigate any new data that have been published and to re-evaluate their previous views, and in particular consider the question “Is there evidence of exposure to chemical contaminants in cabin air that could have long-term health impacts, either from acute exposures or due to long-term low level exposures including mixtures, e.g. of volatile organic compounds (VOCs)?”.
1.167 In 2022, the Committee considered papers on an updated literature search on the potential health risks from organophosphate exposure in aircraft cabin air, an assessment of the concentrations of VOCs in aircraft cabin air compared with other modes of transport and other work environments, and a paper on carbon monoxide and carbon dioxide in aircraft cabin air.
1.168 Further papers will be considered in 2023, before the Committee publishes an updated position.
COT FSA Paving the way for a UK Roadmap: Development, Validation and Regulatory Acceptance of New Approach Methodologies (NAMs) in Chemical Risk Assessment – Development of a UK road map and Workshop Report
1.169 The FSA and COT are developing a UK roadmap towards acceptance and integration of New Approach Methodologies in chemical risk assessment, including predictive toxicology methods using computer modelling, into safety and risk assessments for regulatory decision making. The first draft of the road map was discussed in June 2021.
1.170 A 2-day workshop was then held in October 2021 with the intention of gaining insights from a variety of perspectives to help develop the COT FSA UK Roadmap
1.171 The aim of the workshop was to receive insights, comments and ideas from a wide variety of stakeholders, industry, academia and government, on the roadmap. The idea was to develop it into a useful and engaging document that is of value to more than just the FSA and COT. The workshop addressed issues such as: what might be holding back the progress of NAMs being used in the regulatory space, including a range of areas such as socio-technical barriers, regulatory frameworks and current legislation.
1.172 Members were content with the first draft of the workshop report. Some suggestions on restructuring the introduction were made along with some minor edits.
1.173 The finalised report will be published next year. A third draft version of the roadmap will be published in 2023.
Other Committee Activities Joint Expert Groups and Presentations
Assurance of Joint Expert Group opinions
1.174 The Joint Expert Groups (JEGs) were established by the FSA to assess applications for the authorisations of regulated products that were previously authorised by the European Food Safety Authority (EFSA). The three JEGS were FCM JEG which covers food contact materials, AFFAJEG which has responsibility for animal feed and feed additives, and AEJEG which has responsibility for food additives, enzymes and other regulated products. The COT provides support, challenge and assurance to the work of the three JEGS as set out below. In 2022, AFFA JEG was superceded by the reconstitution of the Advisory Committee on Animal Feeding stuffs (ACAF).
Draft Opinion on the extension of use of polyglycerol polyricinoleate
1.175 The COT considered a Risk Assessment prepared by the Joint Expert Group on Additives, Enzymes and other Regulated Products (AEJEG) regarding a n Application for the extension of use of PGPR in edible ices and emulsified sauces (RP217).
1.176 This item was reserved as it covers a draft AE JEG opinion on an application for the extension of use of the additive polyglycerol polyricinoleate, this is treated as draft policy.
1.177 A statement will be published in 2023.
Draft Opinion on the safety of the extension of use of mono- and di- glycerides (E471) for use as a surface treatment of fresh fruits and vegetables
1.178 The COT considered a Risk Assessment prepared by the AEJEG regarding an Application for the extension of use of mono- and di- glycerides for use as a surface treatment of fresh fruits and vegetables.
1.179 This item is currently reserved as it covers a draft AE JEG opinion on an application for the extension of use of the additive E471, this is treated as draft policy.
1.180 A statement will be published in 2023.
Evaluation of Smoke Flavourings Renewals
1.181 Smoke flavourings are covered by Retained EU Regulation 2065/2003 and therefore need to be authorised before they can be placed on the market in Great Britain (GB). Smoke flavouring primary product authorisations are applicant specific and are valid for 10 years. The current authorisations end on January 2024.
1.182 The FSA has received 8 applications requesting a renewal of the authorisation of smoke flavourings in June 2022, which will be evaluated by the AEJEG. The COT have been kept updated on the progress of these applications.
1.183 The AEJEG meetings for the evaluation of these Applications will commence in the first quarter of 2023.
1.184 This item was discussed as reserved business.
Presentations
UK legislation on Food Contact Materials – an overview – Presentation by FSA FCM policy team
1.185 In light of COT discussions on Biologically-Based Food Contact Materials such as bamboo composites and chitosan as well as anticipated items on ocean bound plastic (OBP) and the COT’s remit to review the output of the Joint Expert Group on Food Contact Materials (FCM JEG), it was considered that an overview of the regulations covering food contact materials would be beneficial.
1.186 FSA policy colleagues provided a brief overview of the overarching food contact material legislation. This included a summary of the enforcing regulations for the UK, which are the Materials and Articles in Contact with Food Regulations 2012 (as amended). The regulations for Great Britain (England, Wales and Scotland)
enforce retained Regulation 1935/2004 (“the framework regulation”) and 10/2011 (“the plastics regulation”), with the current EU Regulations continuing to be applicable in Northern Ireland under the terms of the Northern Ireland Protocol.
1.187 All bio-based food contact materials need to meet the requirements under the retained framework regulation, including good manufacturing practice requirements. Depending on their composition some bio-based food contact materials are additionally required to adhere to the requirements under the retained plastics regulation. Finally, bio-based food contact materials are not regulated products in themselves but applications for such substances may need to be made should the business operator wish to use it in a material that falls under the scope of the plastics regulation.
1.188 Advanced materials may be categorised as active and intelligent materials and therefore would need to meet the additional requirements under retained Regulation 450/2009 (“the active & intelligent materials regulation”). Business operators have a responsibility to ensure that they are aware of the individual components of a material or article and are adhering to the requirements of the relevant regulations. Should the individual components of a material or article not fall under the scope of the additional measures, the default is that it must meet the catch-all framework and good manufacturing requirements. However, the plastics regulation does include multi-component plastic containing materials.
1.189 The EU would be implementing (and since have in October 2022) a new recycled plastics regulation and also have new proposals for legislation on FCMs in general, with a consultation running until the end of January 2023. The FSA will consider appropriate options regarding the updating of retained legislation following the EU proposals. This will provide clarity to operators if they are placing material on the UK or EU markets or both. Environmental considerations are also being taken into account as are other legitimate factors. Ultimately however, the legislation has to ensure that products placed on the market are safe for consumers with no adverse health implications.
1.190 Following the presentation, the Committee discussed the practical implications of regulations for testing that needs to be carried out for a new bio- based material. It was noted that a number of steps would need to be adhered to by the business operator given that the material is unlikely to have been previously used in a food contact material scenario). If the material is expected to be used, for example, in multiple material types, different food contact applications or are multifunctional, business operators will need to ensure that they are carrying out appropriate due diligence. They are responsible for ensuring that final products have undergone the appropriate testing and are safe in expected use.
1.191 The Committee acknowledged that while not directly the topic of the discussion, in some situations, i.e. for non-food applications, the food contact regulations may not be entirely applicable for the product produced and therefore, a cross-cutting approach might be needed (examples such as medical devices and biocidal products).
1.192 There continues to be close collaboration between FCM policy at the FSA and other Government Departments, allowing the business operator to be signposted to the relevant Department.
PhD Student and Postdoctoral Fellow presentations
1.193 The FSA and COT have been considering New Approach Methodologies (NAMs) in order to understand the best scientific methodologies available for use in the risk assessment of chemicals, and to consider how these can be incorporated and accepted in a regulatory context.
1.194 In 2021, the FSA started funding a computational toxicology postdoctoral
Fellow at the University of Birmingham and a PhD Student at King’s College London as part of their Interdisciplinary Doctoral Program (LIDo-TOX AI). The Fellow and PhD student have been working alongside other Government Departments to understand how NAMs will improve indicative levels of safety in chemical risk assessment.
1.195 In addition, these new partnerships have helped with networking, research collaboration, training opportunities and other activities in this area. The Fellowship and studentship also compliment the work set out in the COT FSA UK Roadmap towards (see paragraph 1.169) using NAMs in chemical risk assessment.
1.196 The Postdoctoral Fellow and the PhD student prepared a yearly review and gave presentations to the Committee on their progress to date.
1.197 The Postdoctoral fellow presented two case studies. The first of these focused on the plasticiser di-2-ethylhexyl terephthalate (DEHTP). The main objective was to derive a health-based guidance value. Concentration-response data obtained from ToxCast studies, via the Chemicals Dashboard (US Environmental Protection Agency (EPA)), were used. The second case study had, as chemical of choice, a perfluorinated substance, perfluorooctanoic acid (PFOA). The main objective was to integrate an in silico workflow with transcriptomics data to derive a health-based guidance value for PFOA that could be compared with that previously recommended by EFSA. Transcriptomics data published by Health Canada were used as a data source from in vitro exposures of Human Liver Microtissues (a commercial preparation of spheroids comprising primary hepatocytes and Kupffer cells) to PFOA.
1.198 The PhD student presented on the hybrid Quantitative Structure Activity Relationship (QSAR) model of mutagenicity developed by the Kings College team, which is, on average, 78% accurate at predicting mutagenicity. The hybrid model consists of two constituent QSAR models which individually are approximately 70% accurate on average. The first QSAR model used molecular fingerprint- based similarity index calculations, whereas the second QSAR model used molecular fragmentation, to identify pro-mutagenic characteristics. Principal component analysis (PCA) was successfully used to identify the key determinants of the predictions.
1.199 The COT Members were impressed with the progress to date and gave feedback to the fellow and PhD student.
Opportunities and outlook for UK food and Chemicals regulation post EU exit Workshop
1.200 The COT, UKHSA and FSA organised a workshop in July 2022 held in Liverpool on “Opportunities and outlook for UK food and Chemicals regulation post EU exit”.
1.201 The workshop was to build on the successful: Royal Society of Chemistry (RSC) Workshop of 2019 : Drivers and scope for a UK chemicals framework.
1.202 The 2019 RSC workshop examined where chemicals regulation might be in the post EU exit landscape in the UK and the opportunities that might be realised from that.
1.203 From the 2019 workshop a number of actions were suggested.
1.204 After three intervening years (2022), several global events have impacted the economy and regulation in the UK including the post EU exit environment. In light of these events, the COT considered it would be timely to have a second workshop to review what has been achieved and what still needs to be done to realise the full potential of EU exit.
1.205 The purpose of the workshop was to review the food and chemical regulatory landscape; its transfer to the UK; future UK development (REACH) and divergence (drivers and supporting science); identify challenges and opportunities to consider where new structures and investment are required to realise and address these.
1.206 A workshop report will follow in 2023.
Working Groups
SETE
Report of the Synthesis and Integration of Epidemiological and Toxicological Evidence Subgroup (SETE) of the Committee on Toxicity and the Committee on Carcinogenicity
1.207 The UK Committees on Toxicity (COT) and on Carcinogenicity (COC) regularly review epidemiological and toxicological evidence in their risk assessments. There is, therefore, a need for guidance on the approaches used by the Committees to integrate these evidence streams, both for scientific consistency and to ensure public transparency. To that end, the Committees established the Synthesising and Integration of Epidemiological and Toxicological Evidence Subgroup (SETE) to review and document current practice and provide applicable guidance.
1.208 SETE recognised that issues on which advice from the Committees is sought varies considerably and hence the guidance proposed should be sufficiently flexible to address this.
1.209 Scoping and problem formulation were identified as the crucial first step in the process. This ensures the right questions are asked, helps make the most efficient use of resources and identifies the most appropriate approaches to use in the assessment. An established system or guidance to assess the separate/different evidence streams should be followed where feasible. For both epidemiological and toxicological evidence, a prescriptive checklist or scoring approach is not recommended. However, identifying the strengths and weaknesses of studies is important. The decision-making process should be robust, transparent, evidence- based, defensible and documented, but equally importantly, it should be easy to use. Collaboration and ongoing dialogue between epidemiologists, exposure experts and toxicologists are strongly advised. Information on mode of action (MOA) can be invaluable for evidence integration as it underpins weight of evidence considerations by providing the mechanistic link between empirical observation and biological plausibility.
1.210 All lines of evidence should be considered, with no pre-existing hierarchy. One way to clearly depict the influence of the different lines of evidence on causality is via visual representation (Figure 1).
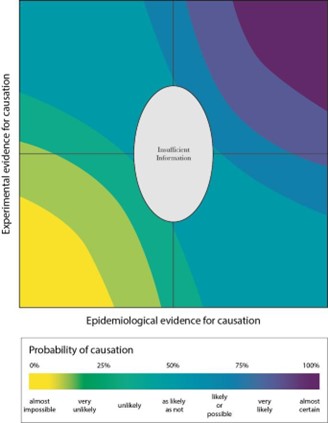
The figure shows a visual representation of the integration of toxicological and epidemiological evidence. It is depicted as an multi coloured image with 2 axis. The vertical axis is: Experimental evidence for causation and the horizontal axis is: Epidemiological evidence for causation. Underneath the image is a small table showing the colour spectrum that relates to the probability of causation.
Figure 1: Example for the visual representation of the likelihood of a causal relationship, considering both epidemiological and toxicological data.
1.211 Decisions on whether there is sufficient information to reach a conclusion or whether a causal relationship in humans is more likely or unlikely can be reached based on where the causal relationship appears on a graph. It is important to begin with the initial estimate of causal relationship at the centre of the graph. Depending on whether the toxicological, mechanistic or epidemiological evidence assessed supports or discounts (or has no clear influence on) a conclusion of causality, placement on the graph is then moved accordingly, either in a positive or negative direction. The movement is influenced by several factors, including the strength or weakness of the evidence, any relative weighing given to epidemiological and toxicological studies and the uncertainties associated with the data. As more information is included in the process and/or becomes available, the placement of the toxicological and/or epidemiological evidence can be easily adjusted and the impact on any possible conclusion easily seen.
1.212 In contrast to other approaches, the above visualisation aims to provide a pictorial representation of the consensus views of a Committee on the influence of the different lines of evidence on causation, assessed by debate and agreement of scientific experts. In this way, it provides a more objective means of collating the views of the Committee and communicating the agreed conclusion of a Committee on the likelihood of causation.
1.213 The conclusion should be stated, with an estimate of the overall uncertainty and, where appropriate, guidance on how data gaps could be filled.
1.214 The full SETE report and guidance document (Annex 1) can be found at: SETE | Committee on Toxicity (food.gov.uk) the guidance will be trialled by the COT for 2 years and then reviewed.
Joint SACN/COT Working Group on Plant Based Drinks
1.216 The Office of Health Improvement and Disparities (OHID) (previously Public Health England) and the FSA received an increasing number of enquiries regarding the use of plant-based drinks in the diets of infants and young children aged 6 months to 5 years of age.
1.217 Current UK government advice regarding the use of plant-based drinks for infants and young children is that unsweetened calcium-fortified plant-based drinks, such as soya, oat and almond drinks, can be given to children from the age of 12 months as part of a healthy balanced diet; however, rice drinks should not be given due to the levels of arsenic in these products.
1.218 In 2021, the COT was asked to consider the potential risks posed by soya, almond and oat drinks consumed in the diets of these age groups. A COT Statement was published in 2021.
1.219 Overall the Committee concluded that neither the safety of these drinks, nor the suitability of the current guidance, could be confirmed from a toxicological perspective. The Members agreed that, in addition to potential toxicological concerns, consideration of nutritional issues would also be required to assess whether it was necessary to issue additional advice on the consumption of plant- based drinks in children aged 6 months to 5 years of age. As a result, a joint SACN/COT Working Group was established in 2021, to consider the benefits and risks of plant-based drinks in diets across all life stages.
1.220 In 2022, a call for evidence was issued which aimed to seek evidence with regards to specific aspects of nutrition, safety and toxicity of plant based drinks. Details on the call for information can be found in the following link: Call for Evidence
1.221 The Joint Working Group considered the information received in response to this call for evidence, the COT Opinions on plant based drinks and cow’s milk as well as exposure information and utilised the Benefit-Risk Analysis for Foods (BRAFO) framework in order to compare the health risks and benefits of plant based drinks.
1.222 It is hoped that the report will be published in 2023.
Joint ACNFP/COT Working Group on Cannabidiol (CBD)
1.223 A joint Working Group has been established to review the data on cannabidiol (CBD) submitted as a part of the novel foods applications process.
1.224 The first meeting of the ACNFP/COT subcommittee was held in July and considered the toxicology datasets collated for CBD isolate applications and ultimately concluded that a list of toxicological uncertainties must be tackled before opinions on the safety of CBD isolates can be made.
1.225 The next meeting was held in September and the main topic of discussion was an in-depth review of the data on CBD isolates and synthetic CBD products. By using a refined but detailed table format, the Secretariat hopes to prompt further discussion amongst the subcommittee members. This will inform the next steps to support the review of dossiers in this group by the ACNFP.
2022 Membership of the Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment
Chair
Professor Alan Boobis OBE, PhD, FBTS, FBPhS
Emeritus Professor of Toxicology in the Faculty of Medicine at Imperial College London.
Members
Dr Phil Botham BSc, PhD
Principal Science Advisor at Syngenta (part time).
Ms Jane Case
Lay Member.
Dr Stella Cochrane BSc PhD
Science Leader for Allergy and Immunology in Unilever’s Safety and Environmental Assurance Centre.
Dr James Coulson BSc MBBCh Dip Med Tox Dip Therapeutics LLM MD FRCP FRCPE ERT
Clinical Reader at Cardiff University, Honorary Professor in Clinical Pharmacology and Toxicology, Cardiff Metropolitan University, Honorary Consultant Physician, Clinical Pharmacologist and Toxicologist, Cardiff & Vale University Health Board.
Dr René Crevel
Director, René Crevel Consulting Limited. (Until March 2022)
Dr Silvia Gratz (from 31st of May)
Senior Research Fellow at the Rowett Institute, University of Aberdeen.
Dr Caroline Harris PhD, CChem, FRSC (Until March 2022)
Practice Director and Principal Scientist, Exponent International Ltd. Term expire
Professor Thorhallur I. Halldorsson
Professor at the Faculty of Food Science and Nutrition at the University of Iceland.
Professor Gary Hutchison
Dean of Applied Sciences at Edinburgh Napier University, with responsibility for Life Sciences, Social Sciences, Psychology, Teacher Education and Sports Exercise and Health Sciences.
Dr Sarah Judge BSc, PhD.
Lecturer in Pharmacology in the School of Biomedical, Nutritional and Sport Sciences at Newcastle University.
Professor Gunter Kuhnle
Professor of Nutrition and Food Science, University of Reading
Dr David Lovell
Emeritus Reader in Medical Statistics at St George’s Medical School, University of London.
Professor Shirley Price
Emerita Professor of Toxicology at the University of Surrey.
Dr Mac Provan
Director of Regulatory Science Ltd.
Ms Juliet Rix
Lay Member.
Dr Michael Routledge
Associate Professor of Environmental Toxicology in the School of Medicine at Leeds.
Dr Cheryl Scudamore
RCVS Specialist in Veterinary Pathology (laboratory animals) working as independent consultant in experimental and toxicological pathology.
Dr Natalie Thatcher
Mondelēz International.
Professor Mireille Toledano
Chair in Perinatal and Paediatric Environmental Epidemiology, Faculty of Medicine, School of Public Health, Imperial College London.
Dr Simon Wilkinson
Senior Lecturer in Pharmacology in the School of Biomedical, Nutritional and Sports Sciences at Newcastle University.
Professor Philippe Wilson
Professor of Animal Science and Bioinformatics, Nottingham Trent University, and Head of Conservation at the Rare Breeds Survival Trust.
Professor Matthew Wright BSc, PhD
Professor of Toxicology, Institute of Cellular Medicine, Newcastle University.
Professor Maged Younes
Independent expert on toxicology and biochemical pharmacology.
Secretariat
Ms Catherine Mulholland BSc (Hons), ERT Scientific Secretary Ms Britta Gadeberg BSc (Hons) MSc Scientific Secretary – PHE Dr David Gott BSc (Hons) PhD
Dr Alexander Cooper BSc (Hons) MSc PhD
Dr Barbara Doerr BSc (Hons) MSc PhD
Dr Douglas Hedley BSc (Hons) MSc PhD (until February 2022)
Ms Jocelyn Frimpong Manso BSc (Hons) MSc
Ms Cleanncy Hoppie BSc (Hons) MSc
Mr Barry Maycock BSc (Hons) MSc
Dr Olivia Osborne BSc (Hons) (Exon) PhD ERT
Ms Claire Potter BSc (Hons) MSc ERT
Dr Joseph Shavila BSc (Hons) MSc PhD
Ms Chloe Thomas BSc (Hons) (until April 2021)
Ms Sabrina Thomas BSc (Hons) MSc Ms Chara Tsoulli BSc (Hons) MSc Ms Ms Frederique Uy BSc (Hons) MSc Miss Sophy Wells
Dr Gaetana Spedalieri
Mr Thomas Hornsby BSc (Hons) MSc
Mr Lawrence Finn BSc (Hons) MSc
Ms Gail Drummond BSc (Hons) MSc, LLB, PG Dip (law)
Dr Emily Hudson BSc (Hons) Mres
Dr David Kovacic
Declaration of members interests during the period of this report
Professor Alan Boobis OBE, PhD, FBTS, FBPhS
|
Personal Interest |
Employee: Imperial College London, Department of Medicine (retired June 2017, part-time appointment from Aug 2017-May 2019). Full retiral June 2019. Emeritus Professor of Imperial College London, National Heart & Lung Institute. |
|
Personal Interest |
Membership: ILSI & ILSI,HESI Board of Trustees ILSI Europe. Board of Directors Science Advisory Board of Swiss Centre for Applied Human Toxicology. Dept. of Health Committee on the Medical Effects of Air Pollutants WHO/FAO JMPR. WHO/FAO JECFA (vet). WHO TobReg. WG10 TC126 (Intense Machine- smoking Regime for Testing Cigarettes). EUROTOX. British Pharmacological Society, British Toxicology Society, Society of Toxicology (USA). Royal Society of Biology (until 2017). Michigan State University MSU Center for Research on Ingredient Safety (CRIS) (External Advisory Committee). Agency for Innovations in Food and Chemical Safety Programme. Science, Technology and Research, Singapore (A*STAR) (Scientific Advisory Board). |
|
Non Personal Interest |
None. |
Dr Phil Botham
|
Personal Interest |
Employee: Syngenta - Principal Science Advisor (part time). |
|
Personal Interest |
Shareholder: AstraZeneca, Regulatory Science Associates(Part, Time Consultant). |
|
Personal Interest |
Membership: British Toxicology Society, Society of Toxicology (USA), European Centre for Ecotoxicology and Toxicology of Chemicals Scientific Committee, European Crop Protection Association Toxicology Expert Group, Crop Life International Human Health Steering Team. |
|
Non-Personal Interest |
None. |
Ms Jane Case
|
Personal Interest |
Employee: Company Secretary of Muse Interiors Stevens & Bolton LLP (as Jane Hughes). |
|
Personal Interest |
Membership: None. |
|
Personal Interest |
Shareholder: Standard Life Santander |
|
Non-Personal Interest |
None. |
Dr Stella Cochrane
|
Personal Interest |
Employee: Unilever. |
|
Personal Interest |
Membership / Affiliation: Unilever representative on the UK FDF Allergen Steering Group (Deputy Chair), FDE Allergen Group and University of Nebraska Food Allergy Research & Resources Board. |
|
Personal Interest |
Shareholder: Unilever. |
|
Non-Personal Interest |
None. |
Dr James Coulson
|
Personal Interest |
Employee: Cardiff University, Director of Medical, Scientific and Toxicology Consultancy Ltd. |
|
Personal Interest |
Membership: British Medical Association, British Pharmacology Society, British Toxicology Society National Trust, Royal College of Physicians of London. |
|
Non-Personal Interest |
None. |
Dr René Crevel
|
Personal Interest |
Consultant: Réne Crevel consulting. |
|
Personal Interest |
Membership/affiliation: ILSI Food Allergy Task Force: Chair. |
|
Personal Interest |
Shareholder: Unilever, Centrica, BG Group,
National Grid, Lloyds. |
|
Non-Personal Interest |
None. |
Professor Thorhallur Ingi Halldorsson
|
Personal Interest |
Employee: Faculty of Food Science and Nutrition, University of Iceland. |
|
Personal Interest |
Membership: European Food Safety Authority - Scientific committee and various working groups. Nordic Council of Ministers - revision of the 2022 Nordic Nutrition Recommendation). Icelandic Risk Assessment Committee for Food, Feed, Fertilizers and Seeds (IRAC) – occasional expert work. The Nutricia Research Foundation – review of applications once a year. The Icelandic Research Found (RANNIS) – occasional member of different expert panels. |
|
Non-Personal Interest |
None. |
Dr Caroline Harris
|
Personal Interest |
Employee: Exponent International Ltd. |
|
Personal Interest |
Membership: International Union of Pure and AppliedChemistry. |
|
Personal Interest |
Shareholder: Exponent Inc. |
|
Personal Interest |
Fellowships: Royal Society of Chemistry. |
|
Non-Personal Interest |
Membership: Expert Committee on Pesticides |
Professor Gary Hutchison
|
Personal Interest |
Employee: Dean of Applied Sciences at Edinburgh Napier University. |
|
Personal Interest |
Membership: Hazardous Substances Advisory Committee DEFRA, British Toxicology Society. |
|
Non-Personal Interest |
None. |
Dr Sarah Judge
|
Personal Interest |
Employee: Newcastle University, Lowcock Properties Ltd. |
|
Personal Interest |
Membership: British Pharmacology Society, British Toxicology Society International Association for Neurotoxicology. |
|
Non-Personal Interest |
Research Funding. |
Professor Gunter Kuhnle
|
Personal Interest |
Employee: Professor of Nutrition and Food Science, University of Reading. |
|
Non-Personal Interest |
None. |
Dr David Lovell
|
Personal Interest |
Employee: Reader in Medical Statistics, St Georges Medical School University of London |
|
Personal Interest |
Membership: HESI GTTC – Biometrics Society, British Toxicology Society Genetics Society, Royal Society of Biology Laboratory Animal Science Association, Royal Statistical Society Statisticians in the Pharmaceutical Industry, United Kingdom Environment Mutagen Society (UKEMS), UK National Centre of Replacement, Refinement and Reduction of Animals in Research(NC3Rs), MRC EMINENT Scientific Review Board. Also, private member of: British Trust of Ornithologists (BTO) English Heritage, Liberty, Campaign of the Protection of Rural England (CPRE), Kew Gardens, Sandwich Bay Bird Observatory Trust(SBBOT), Chelsea Physic Garden, National Trust. |
|
Personal Interest |
Shareholder: National Grid, Pfizer, AstraZeneca (spouse shareholder), National Grid plc (spouse shareholder). |
|
Non-Personal Interest |
None. |
Professor Shirley Price
|
Personal Interest |
Employee: None |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
Trusteeships: Gas Safety Trust |
|
Non-Personal Interest |
Other: I can confirm that as the President of the British Toxicology Society (BTS) I hold a non-personal and non-specific interest in both GSK and AstraZeneca on the Society’s behalf. These non- personal and non-specific interests relate to donations provided by both companies to the British Toxicology Society (BTS) to support their Annual Congress and Education and Training. |
Dr Mac Provan
|
Personal Interest |
Employee: Director of Regulatory Science Ltd. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Ms Juliet Rix
|
Personal Interest |
Employee: None. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Dr Cheryl Scudamore
|
Personal Interest |
Employee: Independent consultant in experimental and toxicological pathology |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Dr Natalie Thatcher
|
Personal Interest |
Employee: Mondelēz International. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Professor Mireille Toledano
|
Personal Interest |
Employee: Marit Mohn Chair in Perinatal & Paediatric Environmental Epidemiology, Imperial College London. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Dr Simon Wilkinson
|
Personal Interest |
Consultancies and other fee-paid work: Consultancy for L’Oreal, Paris. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Professor Phillipe Wilson
|
Personal Interest |
Employee: Nottingham Trent University, Rare Breeds Survival Trust. |
|
Personal Interest |
Membership: None. |
|
Non-Personal Interest |
None. |
Professor Matthew Wright
|
Personal Interest |
Consultancies and Direct Employment: Newcastle University. |
|
Personal Interest |
Membership: British Toxicology Society, Society of Toxicology (US), EFSA FAF Panel. |
|
Personal Interest |
Miscellaneous: Toxicology – Associate Editor. |
|
Non-Personal Interest |
Support by Industry: GSK, Lubrizol. |
Professor Maged Younes
|
Personal Interest |
Employee: Independent expert in toxicology and biochemical pharmacology. |
|
Personal Interest |
Membership: Chair of EFSA ANS panel, Chair Commission on evidence-based methods in risk assessment, Federal Institute for Risk Assessment (BFr), Germany. Society of Toxicology, USA German Society of Experimental and Clinical Pharmacology and Toxicology. Society for Risk Analysis. |
|
Non-Personal Interest |
None. |
Dr Silvia Gratz
|
Personal Interest |
Employee: Rowett Institute, University of Aberdeen |
|
Personal Interest |
Membership: The Nutrition Society (UK) The British Toxicology Society FSA Register of Specialists |
|
Non-Personal Interest |
None. |